Shoulder pain is a very common condition. About 4.7% to 46.7% population suffers from it in one year. The chance of suffering shoulder pain in a lifetime is up to 66.7% and at any point in time, every 4th or 5th person has shoulder pain.
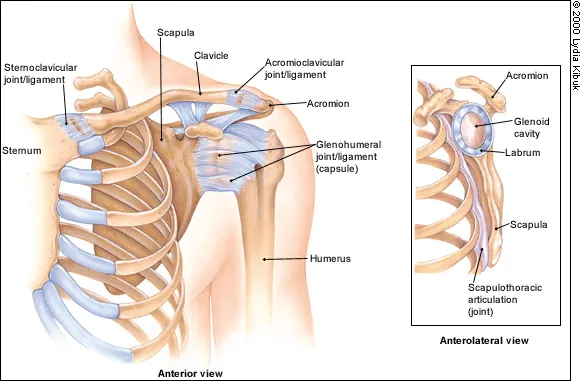
The shoulder is the most movable joint in the body. It is a ball and socket joint with a wide range of mobility; but it is not a single joint, it has 4 joints that work together. These four joints are glenohumeral joint, acromioclavicular joint, thoracoscapular joint and sternoclavicular joint. It is an unstable joint because of the range of motion allowed. It is easily subject to injury because the ball of the upper arm is larger than the shoulder socket that holds it. To remain stable, the shoulder must be anchored by its muscles, tendons, and ligaments, and any of these alone or in combination can be a source of pain.